
Icon® Resin Infiltration
The revolutionary treatment for early enamel and interproximal lesions.
Choose from Icon Smooth Surface or Icon Proximal.
- Aesthetic results on smooth surfaces
- Arrests caries at an early stage
- Preserves healthy tooth structure
- Micro-invasive technology, no anesthesia or drilling
- One quick and simple patient visit
Curion is proud to be an authorized distributor of DMG products in Canada. This product is backed by the manufacturer's warranty.

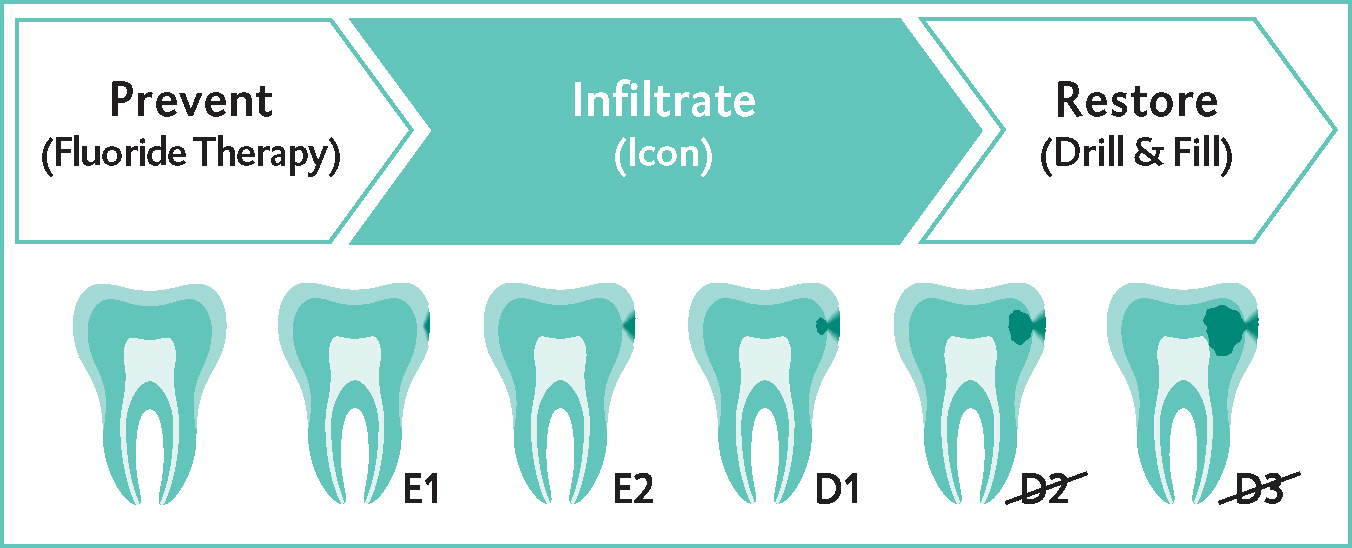
The solution to treating caries while preserving healthy tooth structureUntil now, dental professionals have had only two choices to treat early caries: use fluoride and other treatments to remineralize enamel in the very early stages - or "wait and see" until it's time to "drill and fill." Icon represents a revolutionary new approach to treat incipient caries: a caries infiltrant. This breakthrough micro-invasive technology fills and reinforces demineralized enamel without drilling or anesthesia, up to the first third of dentin (D1). |  |
Why do previous treatments fall short?
- Fluoride therapy isn't always effective in the advanced stages
- Filling almost always sacrifices large amounts of healthy tooth structure
How Icon effectively infiltrates early caries
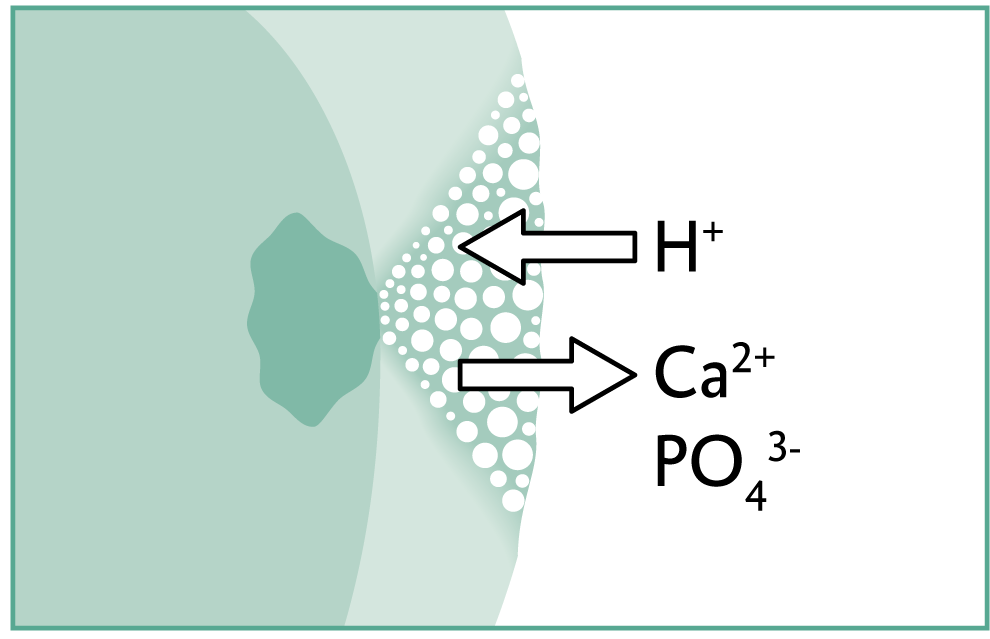 | 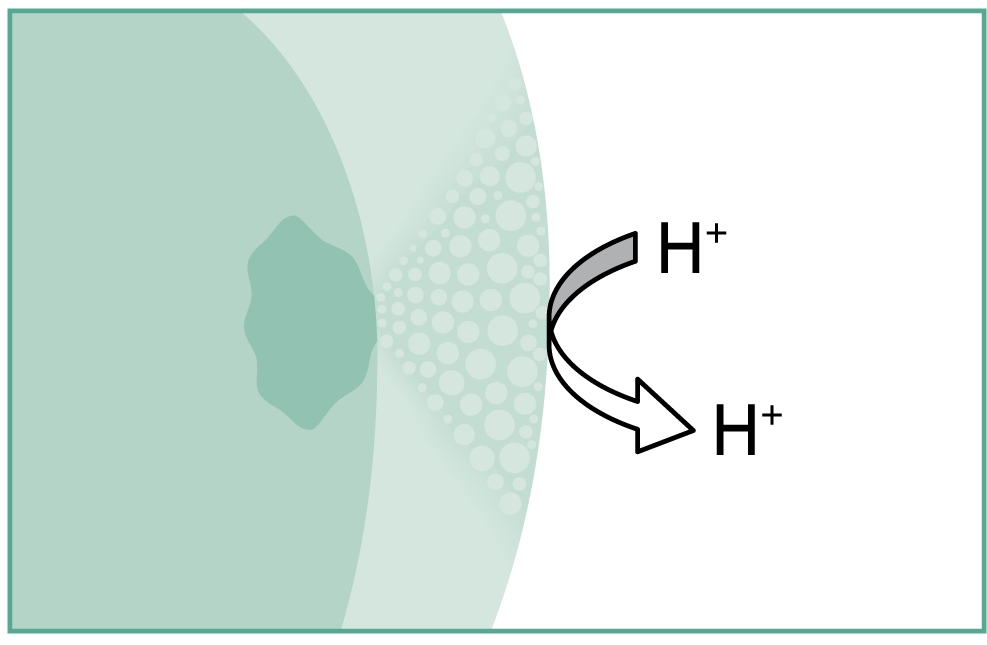 |
| With the onset of caries, cariogenic acids attack the enamel and draw out minerals. | After treatment with Icon, the pore system is closed, blocking the progression of caries. |
 | "White spots are a major issue for my post-orthodontic patients. Icon enables me to remove them in one simple and painless treatment. It's a "wow!" moment for the patient and a significant source of growth for my practice." - Dr. Timothy Hess, DDS |
Icon Smooth Surface Quick Guide
Icon Proximal Quick Guide
Icon Caries Infiltration in 60 seconds
Icon Caries Infiltration: Interview with Dr. Jared Shore
To view all videos, techniques and icon tips, visit DMG Connect here: ICON TECHNIQUES
Frequently Asked Questions
24 months.
Healthy, non-demineralized enamel cannot absorb the infiltrant. However, it can block the progression of an early caries to prevent the need for drilling and filling.
Up to the first third of the dentin (D1).
Caries infiltration is successful even with deciduous teeth and as young as 3 years of age. In general, the safety recommendations in the instructions for use are to be carefully observed and cooperation of the child to undergo a dental treatment is required.
For non-cavitated enamel caries and dentin caries that has not progressed beyond the first third of the dentin.
No. Icon is used in the enamel, and on the dental neck there is only a very thin enamel layer, if at all.
No, because the porous system is different from that of carious demineralization and therefore the result would not be optimal.
No, the infiltration method only works for carious enamel lesions with pore volume.
Smooth surface 4-8, proximal 2
Visually: using the eye, Radiography: bitewing radiographs, or tactile: with a probe
Remove excess when withdrawing the applicator and then clean thoroughly with the air-blowing and suction device. For smooth surface applications cotton rolls are recommended. Before light-curing be sure to clean the interdental spaces (proximal and smooth surface) with dental floss. We recommend Superfloss.
No. Once the infiltrant has penetrated the capillary system it cannot be removed with dental floss or cotton rolls (smooth surfaces).
Afterwards only, especially on smooth surfaces since the entire tooth front was etched.
For the initial cleaning of the tooth the dentist can use the usual prophylaxis pastes.
The actual infiltration treatment includes the following steps:
- Etching for 2 minutes (maybe longer when etching smooth surfaces), rinsing for 30 seconds
- Rinsing with ethanol for 30 seconds, air drying
- First infiltration step for 3 minutes, excess removal, light-curing for 40 seconds
- Second infiltration step for 1 minute, excess removal, light-curing for 40 seconds
About 15 minutes excluding rubber dam placement
By etching with HCl gel we achieve a bond strength of about 20 MPa on enamel.
No, the infiltrant is not radiopaque. Therefore, the documentation in the patient card is very important.
At room temperature up to 25°C. In case of higher ambient temperatures it is recommended to store Icon in the refrigerator.
Check up after 1 – 2 years with a new bitewing radiograph. If the lesion remains unchanged there is no need for further treatment. If the caries progressed a filling restoration should be considered depending on the indication. A follow up appointment should be scheduled one year after the treatment at the earliest, if necessary earlier for risk patients (poor oral hygiene).
Clinical studies revealed that caries treated with Icon will not progress for at least 18 months. These clinical studies are extended and monitored for an additional 5 years.
The infiltrant can easily be removed with a drill.
A Suntest showed that the infiltrant is color-stable both as cured pigment and as infiltrated lesion. In vitro studies with coffee and red wine revealed similar discolorations as with composite fillings. A clinical study on color stability (Cleveland) is currently in progress. Results are expected to be available in October 09.
Yes. Wait a minimum of 2 weeks before bleaching or whitening, after treatment.
The check-up interval is determined by the attending dentist and depends on the individual caries risk of the patient. Please observe general radiation protection guidelines.
We strongly recommend the use of a rubber dam since the area to be infiltrated must be kept absolutely dry for successful treatment (similar to a composite filling). Therefore, the drying step with ethanol is also very important. If the dentist can ensure to keep the area dry even without the use of a rubber dam it is at his/her discretion.
The two-minute etching process removes an enamel layer of 40 µm. (Please note that healthy enamel has a thickness of 1,000 – 1,500 µm.)
No, the application of HCl gel on sufficiently thick enamel is not painful.
Gum areas that come in contact with the HCl gel will turn white but will return to their natural color after about 2 weeks. Since a rubber dam is used for this treatment step though, contact should not occur.
Yes, as long as they are in the pseudo-intact surface layer. The removal of the pseudo-intact surface layer also removes the discolorations embedded therein. In case of insufficient removal the etching step can be repeated locally.
Drying of the teeth to be treated reveals if the etching process was successful, especially when treating smooth surfaces, and facilitates successful penetration of the infiltrant into the lesion body.
No. Due to the permanent moisture in the dentinal tubule Icon cannot infiltrate the dentin. dentin is organic and hydrophilic, the infiltrant is hydrophobic. Therefore, the infiltrant cannot penetrate into the dentin.
Yes, it can be used for lesions up to the first third of the dentin. Due to the permanent moisture in the dentinal tubule, Icon cannot infiltrate the dentin. Dentin is organic and hydrophilic and the Icon Infiltrant is hydrophobic. Therefore, it cannot penetrate into the dentin.
0.45ml = 5.5 rotations: approximal: 1.4 rotations per tooth x 2 teeth x 2 applications. Vestibular (3 smooth surfaces) = 0.92 rotations x 3 teeth x 2 applications
One to two turns of the rotary plunger are recommended so that there is slight excess.
If too much material is dispensed, the Icon-Infiltrant will run over. It is recommended to use a dental mirror during the application. Minimal excess on the surface is recommended.
There is shrinkage, but due to the ratio of free to bonded surface (C factor) it has no negative impact. In order to compensate for the shrinkage during polymerization the application of Icon is repeated (for 1 minute) to fill any voids.
Areas treated with Icon are not visible under black light (only the dentin is fluorescent which is treated only to a small extent, if at all. Enamel is not fluorescent).
The infiltrant is readily compatible with composites since it is also a monomer/composite material.
A sealant is applied as a surface layer onto the enamel surface. This is done mostly on occlusal surfaces (fissure sealing). Fissure sealing is generally used preventively (exception: extended fissure sealing).
Icon penetrates into the enamel, seals the lesion from the inside and does not create a filling margin or a layer on the surface. The infiltration fills an existing pore volume and is thus not preventive.
The wedge in the rotary disk of the plunger shaft helps with the dosing: Generally, 1.5-2 rotations of the plunger shaft are enough to dispense sufficient material. Working with a slight excess is recommended.
Yes, when treating adjacent smooth surfaces per work step several lesions can be treated at the same time with the same applicator.